


Introduction
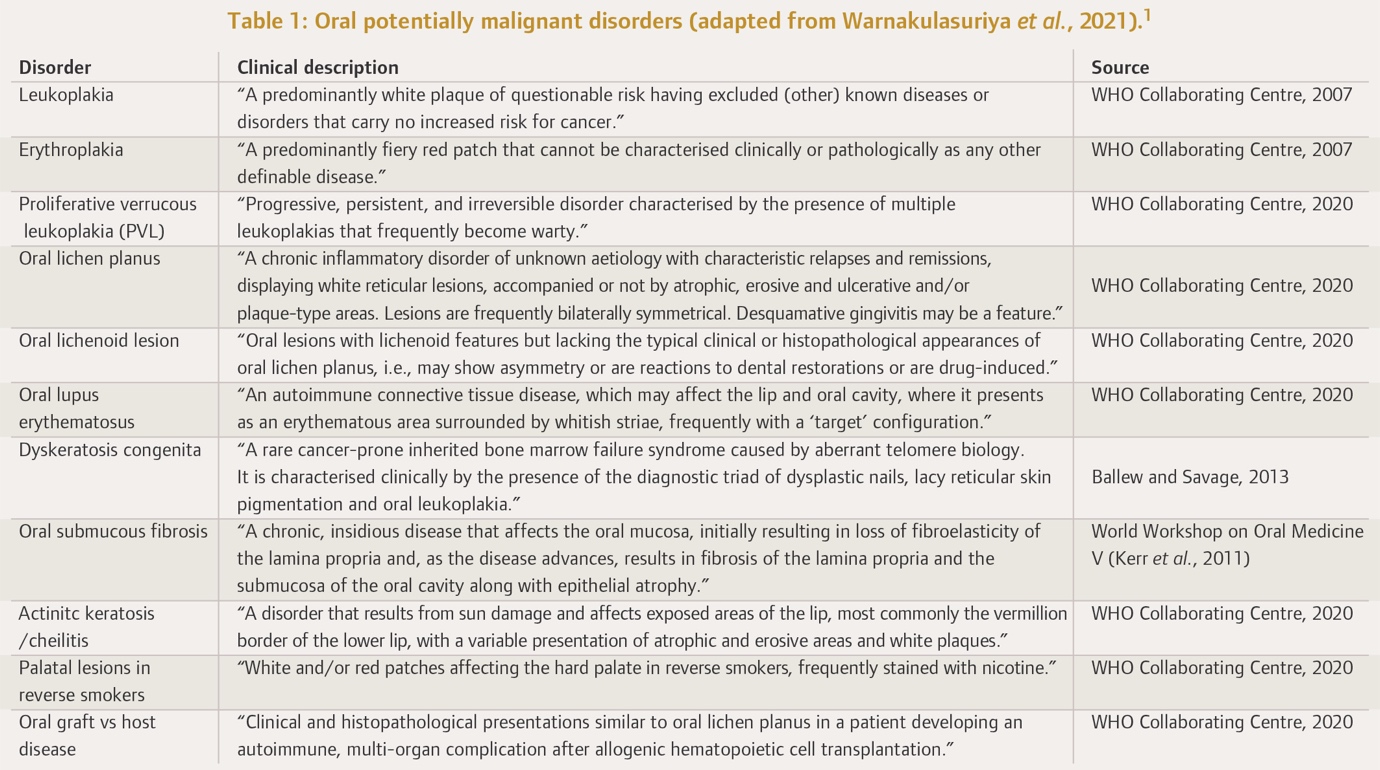
Oral white patches are frequently seen in general dental practice and represent a wide spectrum of possible conditions, with various aetiologies and prognoses, ranging from benign, reactive mucosal disease to oral squamous cell carcinoma (OSCC). Oral leukoplakia is a common cause of such white patches. Oral leukoplakia is defined as a white patch of questionable risk having excluded all (other) potential causes that carries no increased risk of carcinoma.1 Oral leukoplakia is the most common oral potentially malignant disorder (OPMD) (Table 1). The term OPMD refers to any oral mucosal abnormality that is associated with a statistically increased risk of developing oral cancer.1 Given the risk of malignant transformation associated with leukoplakia, it is imperative that general dental practitioners (GDPs) recognise oral leukoplakia and understand the appropriate management of this condition.

Aetiology
The development of oral leukoplakia appears to be multifactorial in nature. However, the definitive cause is unclear. Smoking has been identified as the predominant risk factor, with oral leukoplakia six times more common in smokers.2 Alcohol is recognised as an independent risk factor for oral leukoplakia.3 However, its aetiological role is less clear in oral leukoplakia than in OSCC. Oral leukoplakia also arises in non-smokers and non-alcohol drinkers, suggesting a potential genetic predisposition.4 Betel quid is a significant aetiological factor in Southeast Asia and is responsible for the increased prevalence of oral leukoplakia in this region.
Epidemiology
While reported rates of oral leukoplakia vary among different geographic regions and demographical groups, a recent systematic review and meta-analysis reported a pooled prevalence of 4.11% globally.5 Oral leukoplakia is more commonly seen in men and is increasingly common with age.
Clinical presentation
Oral leukoplakia can affect any part of the oral mucosa, either as solitary or multiple white patches. The sites most commonly affected include the lateral and ventral tongue, buccal mucosa, and floor of the mouth, the latter site being frequently affected in populations with a high prevalence of smoking.6
Oral leukoplakia may be subclassified into homogeneous and non-homogeneous forms. Homogenous oral leukoplakia (Figure 1) is characterised by a predominantly flat, uniform, often well-demarcated white patch, with a consistent surface topography, and it usually lacks symptoms.1 When homogenous oral leukoplakia is found on the floor of the mouth, it can have a distinctive ebbing tide appearance (Figure 2).


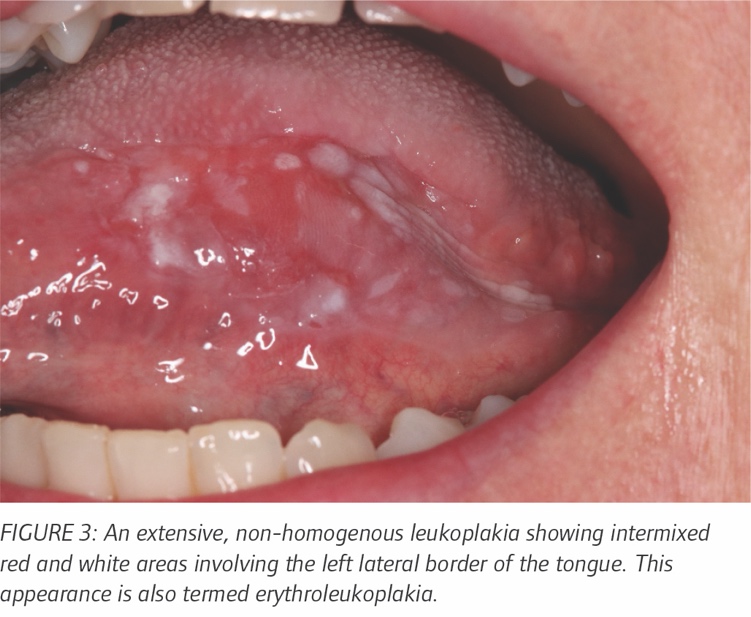
The non-homogeneous form is any white patch that deviates from the above. Non-homogenous oral leukoplakia should be regarded with significant suspicion as it carries a higher risk of malignant transformation than homogenous oral leukoplakia.7 There are several diverse clinical presentations including erythroleukoplakia (Figure 3), which is defined as a mixed white and red patch, but retaining a predominantly white colour. Non-homogenous oral leukoplakia may show focal superficial ulceration and the margins can be more diffuse. Non-homogenous oral leukoplakia with red or ulcerated areas can be symptomatic. Finally, proliferative verrucous leukoplakia (PVL) (Figure 4) is a rare form of oral leukoplakia, characterised by an exophytic, wrinkled, corrugated surface. PVL commonly affects the gingivae, is often multifocal, and is most commonly found in elderly females.


Diagnostic procedures
History and clinical assessment
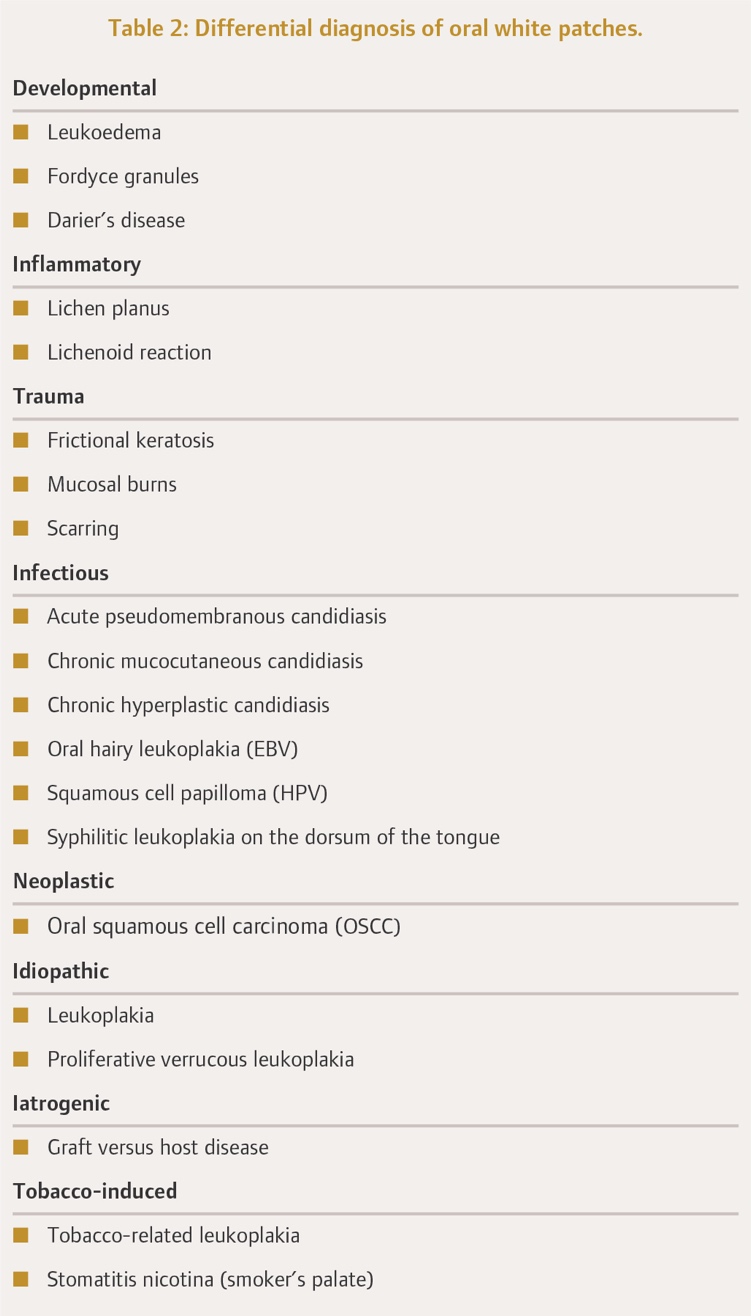
White patches suggest the classic differential diagnostic spectrum, ranging from benign hyperkeratosis to frank carcinoma. Therefore, the first stage in managing a white patch is a comprehensive history and examination to rule out other more common causes (Table 2). Assessment should begin with a history of the patch itself, including its onset and evolution, as well as any associated symptoms, including any pain or bleeding from the site. Patients should be asked about any skin, genital, scalp, or nail involvement, and about joint or muscle pain, which could indicate lichen planus or lupus as possible causes.
An up-to-date medical and social history is essential to identify risk factors for oral leukoplakia. This should include questions relating to a family history of white patches or oral cancer, genetic conditions, and immunosuppression. The medication list should be reviewed to identify if the patient is taking any drugs that can elicit lichenoid reactions. Patients should be asked about past or current smoking habits and, if current smokers, they should be asked details about previous quit attempts, including number of attempts, duration of quit periods, smoking cessation aids used, and triggers for resumption of tobacco. Similarly, alcohol consumption should be quantified, and the use of betel nut queried, as appropriate.

A thorough intra- and extraoral examination is necessary. All cervical lymph nodes should be palpated in case carcinoma is already present and has spread to involve regional lymph nodes. The size and site of the patch should be inspected and noted, as well as its homogeneity. Palpation to assess texture is important, as induration (hardness on palpation) or tethering to tissue planes are early signs of carcinoma, requiring urgent referral. An assessment of the entire oral mucosa and dentition is necessary to identify any other white or red patches, and to identify any possible sources of trauma that could be inducing frictional keratosis. Finally, photographic documentation is essential for monitoring changes in the patch and to aid in triaging patients referred to specialist care.
The clinical findings along with the history must be interpreted by the practitioner to decide the next stage of management. This will most likely involve referral to secondary care. A detailed referral letter using institutional referral proformas, if available, and including clinical photographs of the oral leukoplakia, should be sent to facilitate appropriate triage at the specialist centre. If there is an obvious source of trauma from adjacent teeth or a denture, this should be addressed first, and the area reviewed two to three weeks later. Referral to secondary care should proceed if there is no improvement in the white patch. If there is no obvious cause, then a referral should be made immediately. Of note, white patches on edentulous alveolar ridges are generally due to friction when chewing and can be monitored in general dental practice, only requiring referral if atypical in appearance.
GDPs should also address potential risk factors and encourage smoking cessation and alcohol reduction, if applicable, directing patients to available support services, e.g., HSE Quitline. In this regard, the HSE provides online training to all healthcare professionals in Ireland (Making Every Contact Count; MECC), which provides tools for brief interventions in health promotion.8
Upon receipt of a referral for an oral leukoplakia in a specialist unit, the patient will be assessed and will likely proceed to biopsy. Histological examination is important, firstly to exclude other conditions that can present as a white patch (e.g., lichen planus, chronic hyperplastic candidiasis), and secondly to determine the presence and degree of epithelial dysplasia. Usually, an incisional biopsy is carried out from the most clinically suspicious area of the patch, which will usually correlate with the most severe histological findings. If the oral leukoplakia is small, however (e.g., <5mm), an excisional biopsy may be performed.
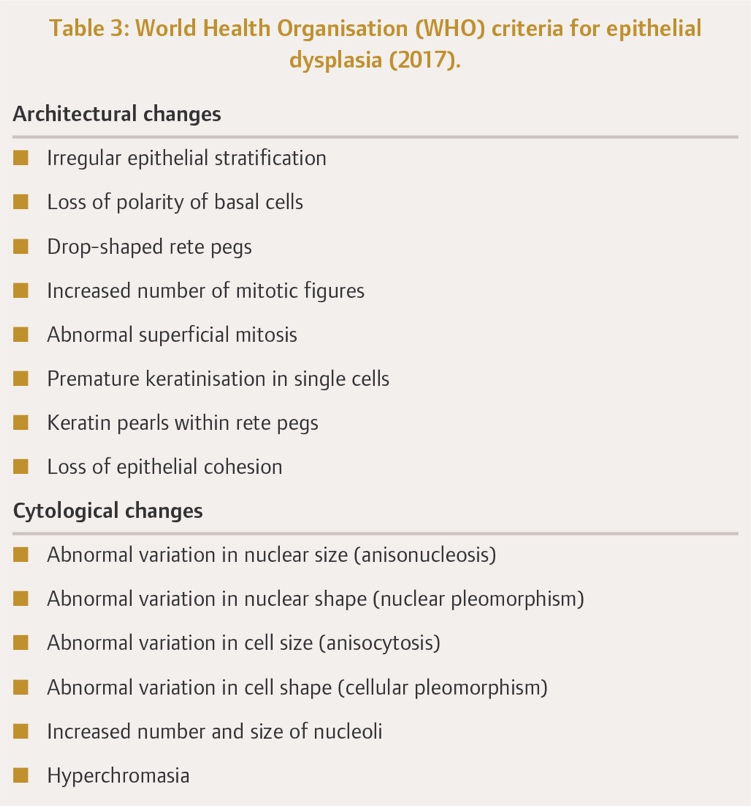
On histopathological examination of oral leukoplakia, hyperkeratinisation is always present, which is responsible for the white appearance of the patch. However, epithelial atrophy and hyperplasia may also be evident. The pathologist will look for the presence of oral epithelial dysplasia (OED), which is a disturbance in the differentiation of the epithelium. Several classification systems have been proposed over the last two decades in an attempt to standardise the reporting of OED. A three-tier grading system proposed by the World Health Organisation (WHO) is used to grade OED as mild, moderate, or severe (Table 3). The most recent iteration of this system has some notable changes, including an absence of the terms ‘squamous hyperplasia’ and ‘carcinoma in situ’, the latter term now being used synonymously with severe OED. Occasionally, an early OSCC is identified on biopsy and then the patient will proceed to definitive cancer management.

Malignant transformation of leukoplakia
Oral leukoplakia is an OPMD and, as such, a common question from patients following a diagnosis of leukoplakia is the risk of transformation into OSCC. The likelihood of malignant transformation cannot be reliably predicted and is patient specific. The pooled proportion of malignant transformation of leukoplakia is estimated at 9.8%.9 While no single factor can reliably determine the risk of carcinoma, several have been highlighted as important predictive factors:
Dysplasia grade
The degree of dysplasia is regarded as the most important determinant for progression to invasive carcinoma,10 with the risk of malignant transformation increasing with increasing degrees of OED.9 Warnakulasuriya et al. (2011) reported 10-year malignant transformation rates (MTRs) of 4.8% and 26.7% for mild dysplasia and severe dysplasia, respectively.11
Non-homogeneity
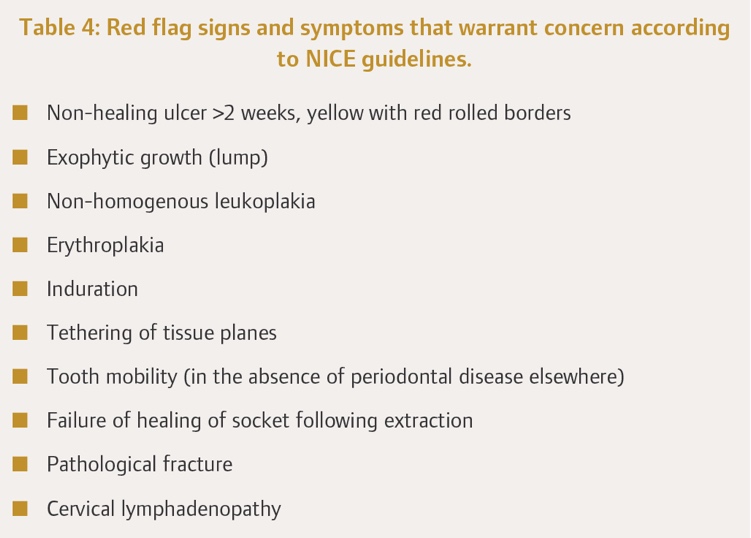
The presence of redness or nodularity in an oral leukoplakia is associated with a greater risk of developing carcinoma9 and these are red flags for GDPs to be aware of, as they require urgent referral (Table 4). PVL in particular has a significantly increased 10-year MTR of 49.5% compared to homogenous oral leukoplakia.12

Site
Floor of the mouth, ventral and lateral tongue, and soft palate oral leukoplakias are at increased risk of malignant transformation compared with those on the buccal mucosa.9
Size
Oral leukoplakias greater than 200mm2 are at greater risk of developing carcinoma.9
Female sex
While oral leukoplakia is more common in males, oral leukoplakias in females are more likely to undergo malignant transformation.6,9
Age
The incidence of malignant transformation increases with age.9
Smoking status
Paradoxically, some studies have found that oral leukoplakias in non-smokers are at increased risk of malignant transformation.13
Management of leukoplakia
General considerations
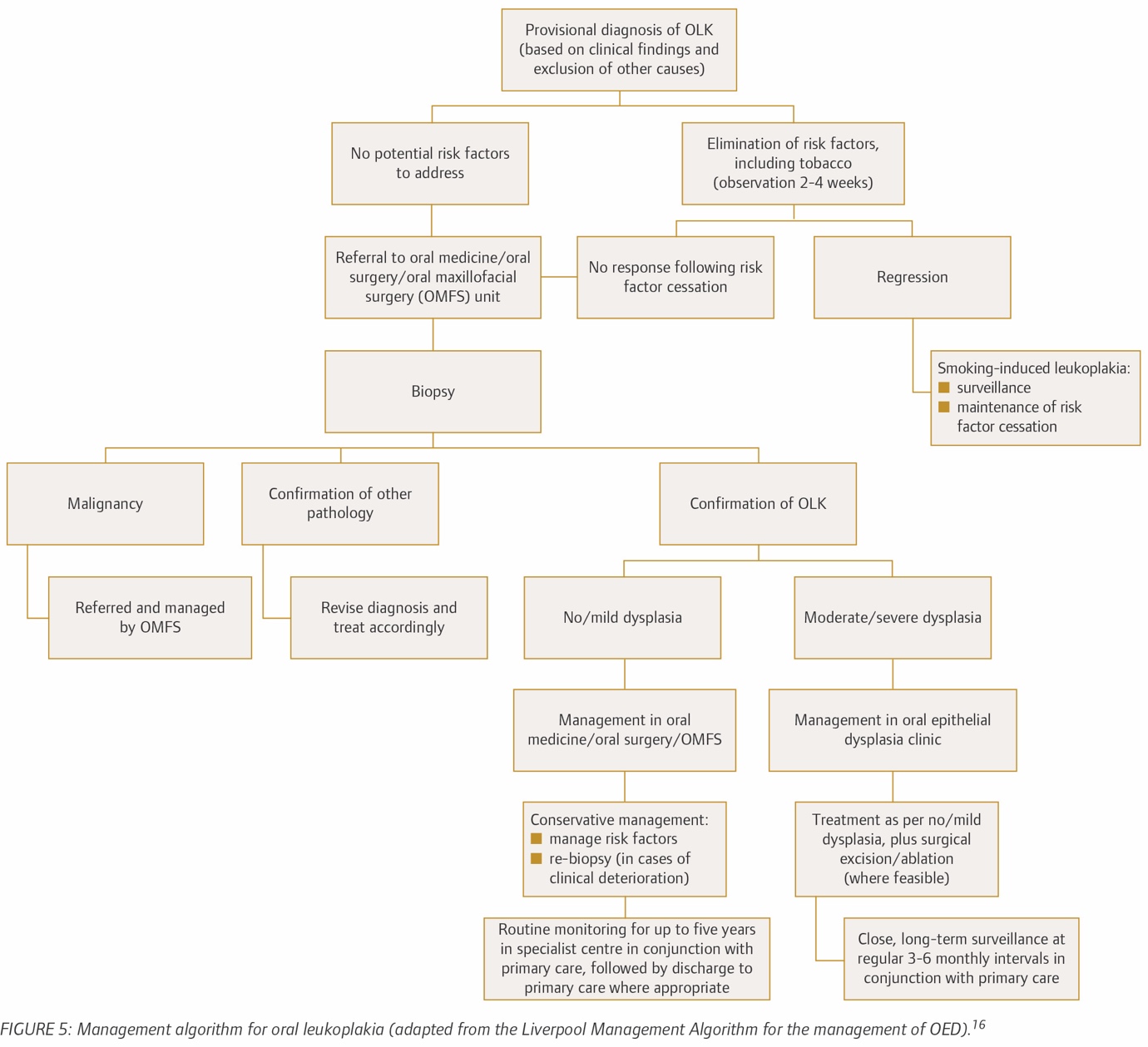
Currently, no consensus exists on the management of oral leukoplakia, and the management algorithm is dictated by a combination of patient, clinical, and histological factors, through a shared decision-making process. The British Association of Head and Neck Oncologists (BAHNO) Head and Neck Cancer Multidisciplinary Management Guidelines offer recommendations for the management of oral leukoplakia.14 This protocol emphasises the use of histological assessment and cessation of risk factors, as well as surgical excision where permissible. A simplified algorithm can be found in Figure 5.
The primary objective for treatment is the prevention of transformation into OSCC, considering the poor prognosis of OSCC and the considerable morbidity associated with its management. While there is an elevated risk of OSCC developing from oral leukoplakia, many leukoplakias do not progress to carcinoma. Unfortunately, it is not possible to reliably predict which patches will undergo malignant transformation and which will not. Therefore, management must be based on individual risk assessment. Given that the degree of OED is at present the most reliable predictor of malignant transformation risk, this is the primary consideration in risk stratifying oral leukoplakias and patients.

Low-risk oral leukoplakias
Oral leukoplakias that demonstrate no/mild OED can often be managed conservatively. This involves addressing known risk factors for malignant transformation, i.e., alcohol and smoking. If a patient has other risk factors, however, the risk may need to be reassessed. Photographs at each review are essential to monitor the evolution of the oral leukoplakia. Surgical removal of areas may be advocated if the dimensions are small.15
High-risk oral leukoplakias
Risk factors must be addressed in patients with oral leukoplakia showing moderate/severe OED, and excision is generally advocated if feasible. Several methods are available. Laser ablation and cryosurgery are not advised, however, as they have the significant disadvantage of causing tissue destruction, so there is no specimen available for histopathological examination. An important factor that must be considered when deciding if surgery is the best option is whether the morbidity likely to arise from the surgery is justified.16 A part or the entirety of the area can be removed, a decision that is often dictated by the size and site of the oral leukoplakia, and the functional status and wishes of the patient. Multifocal oral leukoplakia poses a particular challenge in this regard. A significant advantage of surgical removal of the area includes the benefit of providing the entire specimen for histological analysis, with one study identifying foci of OSCC in 7% of excised oral leukoplakias.17 While surgical excision is the treatment of choice in the presence of moderate or severe OED, 10-35% of cases demonstrate recurrence post excision, particularly if there is dysplasia present at the excision margins or persistence of risk factors.18
While some medical treatments, such as the use of agents either topically or systemically (e.g., anti-inflammatory agents) have been shown to result in oral leukoplakia improvement or resolution, adverse effects and relapse after discontinuation of treatment are exceedingly common.19
Surveillance and follow-up
Patients must be informed that progression of oral leukoplakia to malignancy can occur and that recurrence of oral leukoplakia following excision is possible. Patients should be taught how to perform oral self-checks regularly and to report any changes associated with the oral leukoplakia. Long-term follow-up is advocated, which may even be lifelong.20 GDPs therefore play an important role in the ongoing surveillance of these patients.
There are no strict guidelines on the frequency of follow-up for patients with oral leukoplakia, with periodicity most often dictated by the degree of OED on biopsy. Although there is little evidence to indicate that follow-up of patients with OED has any influence on preventing the development of cancer, regular review facilitates early detection of OSCC in the event of malignant transformation, which is associated with less destructive surgical treatment and a significantly improved long-term prognosis. Given that it may take up to ten years for oral carcinoma to develop from oral leukoplakia, long-term follow-up is considered best practice, at three- to 12-month intervals, depending on the degree of OED and other risk factors.14
Repeat biopsy/biopsies should be carried out in the event of a clinical change in the oral leukoplakia, e.g., development of ulceration, or induration, which could indicate the development of an OSCC. There is no evidence for serial monitoring biopsies in the absence of clinical change.
Challenges with leukoplakia
Oral leukoplakia rarely presents with any symptoms, which can lead to delayed diagnosis. While clinical examination of the oral mucosa has a high sensitivity for the detection of oral leukoplakia (93%), its specificity can be as low as 31%.21 Meticulous screening of all patients for oral leukoplakia and recognising the need to refer to secondary care are essential to allow for early diagnosis, addressing of modifiable risk factors, and further specialist management.
The cessation of tobacco habits and alcohol consumption can result in the resolution of oral leukoplakia and therefore the risk of oral cancer. It has also been shown to reduce the risk of recurrence post excision and the risk of postoperative infection.22 Difficulties with adherence to cessation programmes are a concern for the recurrence or progression of oral leukoplakias, with up to 30% of patients failing to sustain smoking cessation long term.23
Patients with oral leukoplakia are also at increased risk of developing OSCC in other parts of the oral cavity and upper aerodigestive tract due to field change. Field change refers to the concept that cells within the same region have been exposed to the same environmental and genetic influences as the mucosa where the oral leukoplakia has arisen, and so have an increased susceptibility to dysplasia/OSCC. The full extent of the field, however, cannot be assessed histologically,24 and it is not feasible to remove what is clinically normal mucosa throughout the region.
Despite our understanding of the predictive factors associated with the malignant transformation of oral leukoplakia, based on our current knowledge there are no objective measures to determine an individual’s likelihood of transformation to OSCC. Additional challenges arise with the management of multifocal oral leukoplakia, i.e., PVL. Its extensive involvement and persistent spread render it difficult to completely excise. There is also a high rate of recurrence and transformation to OSCC, as mentioned previously, warranting frequent reviews and repeat biopsy procedures in the event of clinical change.
Conclusion
Oral leukoplakia, a common OPMD that is usually asymptomatic, is likely to be encountered in general dental practice. Its clinical importance is derived from its association with the development of OSCC, a disease with high morbidity and mortality. The main strategy in the management of oral leukoplakia is early diagnosis, the addressing of modifiable risk factors, regular surveillance, and surgical management, as dictated by the clinical situation. GDPs are the healthcare practitioners best placed to detect oral leukoplakia, given the volume of patients from various backgrounds encountered daily. An understanding of the aetiology and presentation of oral leukoplakia will place GDPs in a better position to detect this entity, address risk factors, refer appropriately, and participate in its long-term surveillance.