Bishop Score Calculator
Mark Curran M.D. F.A.C.O.G.
The
Bishop Score (also known as
Pelvic Score) is the most commonly used method to rate the readiness of the
cervix for induction of labor. The Bishop Score gives points to 5
measurements of the
pelvic examination dilation, effacement of the cervix, station of the fetus,
consistency of the cervix, and position of the cervix. The calculator
below will calculate a Bishop score
The Bishop’s score was originally developed to predict the
likelihood of a woman entering labor naturally in the
near future. A woman with a low score of 1 would not expected go into
labor for about 3 weeks. A
woman with a higher score score of 10 could be expected to go into
labor within a few days.
Although the Bishop’s score was originally used to evaluate the likelihood of
vaginal delivery in women who have given birth before (multiparous)
it is also now used for women who have never given birth (nulliparous)
who are being considered for induction of labor.
If the Bishop score is 8 or greater the chances of
having a vaginal delivery are good and the cervix is said to be favorable or
"ripe" for induction. If the Bishop score is 6 or less the chances
of having a vaginal delivery are low and the cervix is said to be unfavorable
or "unripe" for induction.
A simplified Bishop score using only dilation, station and
effacement may be as predictive of successful induction as the original
full Bishop score. A simplified Bishop score of 5 had a similar predictive
value of having a successful vaginal delivery as an original Bishop score
of greater than 8.
How The Points Are Assigned
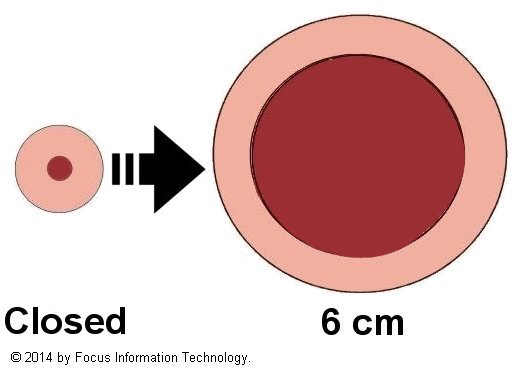
Dilatation
 (Dilation) (Dilation)
The most important element of the Bishop score is dilatation. Dilatation is the
distance the cervix is opened measured in centimeters (cm) . For reference a penny is about 2
cm across. Points are given from 0 to a maximum of
3 points for a cervix dilated to 6 cm or greater.
Effacement
Effacement (also called shortening or thinning) is reported as a percentage from zero percent
(normal length cervix) to 100% or complete (paper thin cervix). Points are given from 0 to a maximum of
3 points for a cervix effaced to 80 % or greater.
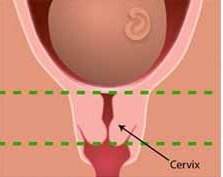 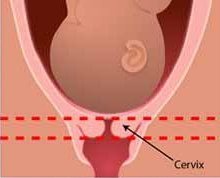
Image credit: National Institutes of Health 2011.
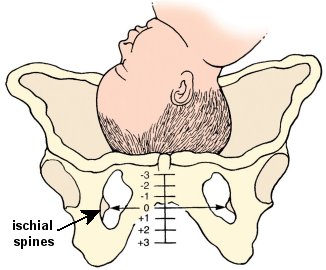
Station
Station is the position of the baby's head relative to the bony projections
of the lower pelvis called the ischial spines. When the baby's head
is at 0 station its head is even with the ischial spines. Stations divides the pelvis above and below the ischial spines into 3rds
Negative numbers indicate that the head is
above the ischial spines. Positive numbers indicate its head is below the
ischial spines.
Points are given from 0 to a maximum of 3
points for a station of 1 + or 2+. |
(c) LifeART / www.fotosearch.com Stock Photography
|
In 1988, the American College of Obstetricians and Gynecologists redefined station
as the level of the leading bony point
of the fetal head at or below the level of the maternal
ischial spines measured in centimeters (0–5 cm).
Consistency
The texture of the cervix on examination.
Firm : The cervix feels hard and rubbery .
Medium: The cervix feels compressible but not soft
Soft : The cervix feels mushy
|
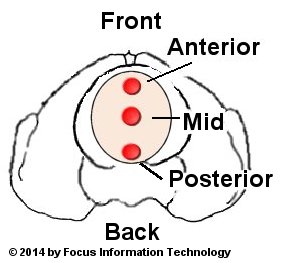
Position
The position of the cervix relative to the fetal head and
maternal pelvis |
 |
Reviewed by Mark Curran, M.D. FACOG
REFERENCES
1. Bishop EH Pelvic scoring for elective induction.Obstet
Gynecol. 1964 Aug;24:266-8. PMID: 14199536
2. .ACOG Practice Bulletin No. 107: Induction of labor.ACOG Committee on
Practice Bulletins -- Obstetrics.Obstet Gynecol. 2009 Aug;114(2 Pt 1):386-97.
PMID: PMID: 19623003
3. Crane JM. Factors predicting labor induction success: a critical analysis.
Clin Obstet Gynecol. 2006 Sep;49(3):573-84. PMID: 16885664
4. Spong CY, et. al. Preventing the first cesarean delivery: summary of a joint
Eunice Kennedy Shriver National Institute of Child Health and Human Development,
Society for Maternal-Fetal Medicine, and American College of Obstetricians and
Gynecologists Workshop. Obstet Gynecol. 2012 Nov;120(5):1181-93. PMID: 23090537
5. Laughon SK, et. al., Using a simplified Bishop score to predict vaginal
delivery Obstet Gynecol. 2011 Apr;117(4):805-11. doi:
10.1097/AOG.0b013e3182114ad2. PMID: 21383643
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3297470/
6.Obstetric Forceps, ACOG committee opinion, no. 59. Washington DC: American
College of Obstetricians and Gynecologists 1988
7. Cunningham FG, Leveno KJ, Bloom SL, et al: Normal Labor and Delivery. In
Williams Obstetrics, 23rd ed., p 392 2010
8.Xenakis EM, et al., Induction of labor in the nineties: conquering the
unfavorable cervix.
Obstet Gynecol. 1997 Aug;90(2):235-9.PMID: 9241300
|
