


A 51-year-old woman with an 8-year history of systemic lupus erythematosus was hospitalized with fever, refractory thrombocytopenia and generalized rash. The patient had previously undergone splenectomy. She had been taking azathioprine and prednisolone daily for more than 1 year. The rash had begun as itchy minor eruptions 3 months previously. Initially, it had been diagnosed as a psoriasiform dermatitis and was treated with topical corticosteroids. After 2 weeks of the corticosteroid therapy, the rash had worsened. The lesions became scaly, lichenified, crusted plaques on her hands (Figure 1), umbilicus, neck, upper back, armpits, inguinal folds and legs.

Figure 1: The hand of a 51-year-old woman with systemic lupus erythematosus, showing cutaneous greasy eruptions caused by Norwegian scabies.
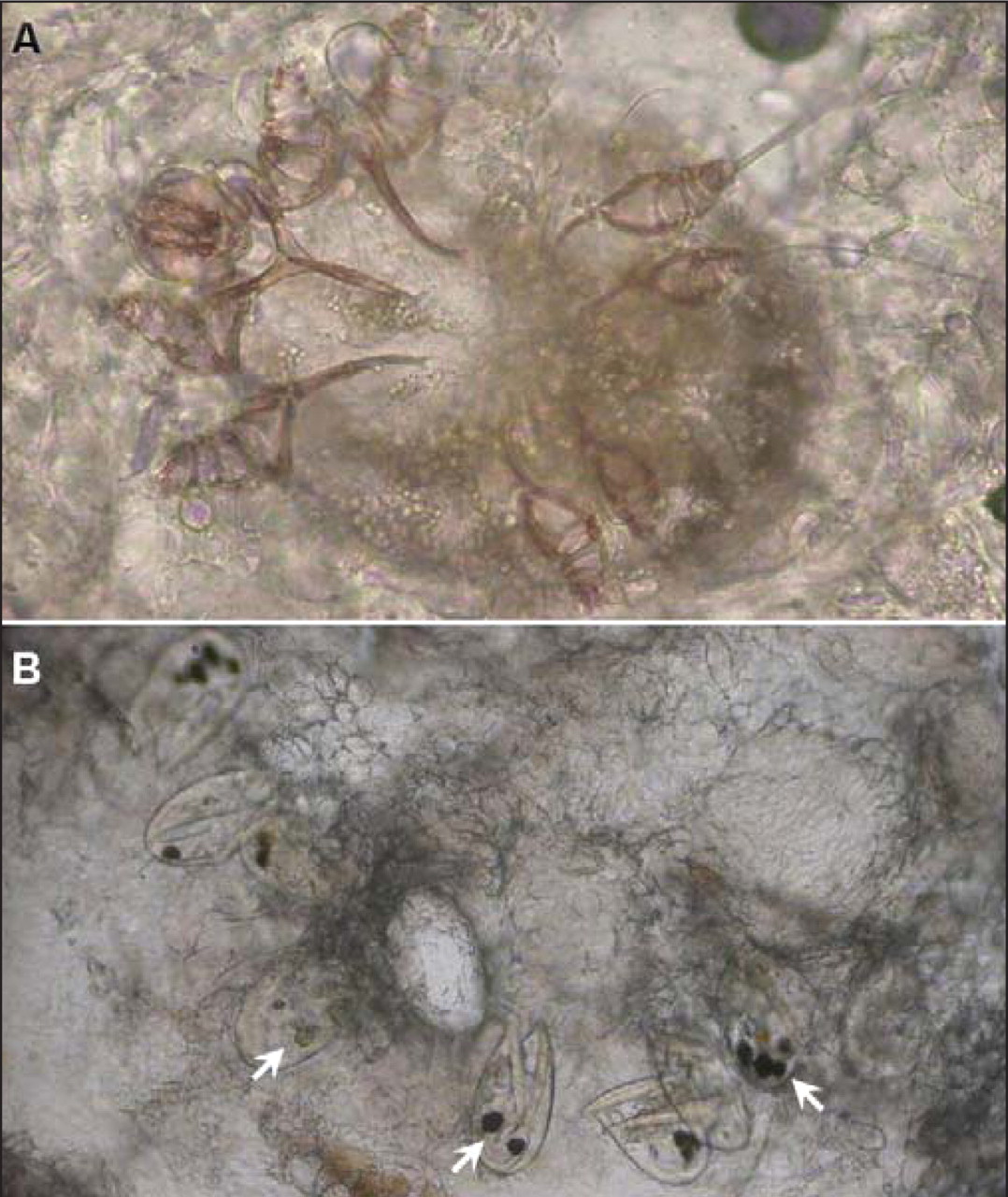
The distribution and appearance of these lesions was consistent with Norwegian (or crusted) scabies. Skin scrapings from the wrist and periumbilical plaques of the patient were examined microscopically. Numerous scabetic mites (Figure 2A), eggs and fecal pellets (also called scybala) (Figure 2B, arrows) were observed, which confirmed the diagnosis. The skin eruptions were treated successfully with application of topical 25% benzyl benzoate lotion for 1 week and removal of the crusts after softening of the scales with vegetable oil.

Figure 2: Microscopic image of skin scrapings showing scabetic mites (A), eggs and fecal pellets (B, arrows).
Crusted Norwegian scabies is highly contagious 1 and may be misdiagnosed as chronic dermatitis. This uncommon, hyperkeratotic form of scabies infestation tends to occur in people who are immunosuppressed or elderly. Outbreaks can occur in institutions. 2,3 Despite its high mite-load, Norwegian scabies may cause only mild discomfort, leading to delay in diagnosis and treatment. Topical scabicides are widely available for treating both classic and atypical scabies. An administration of 2 doses of oral ivermectin (200 μg/kg) given 2 weeks apart is very effective and may be used as a first-line therapy or in combination with topical agents. 2
Footnotes
-
Previously published at www.cmaj.ca on July 20, 2009.
In this issue
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

