The cervix, also called the cervix, is the lower fibromuscular portion of the uterus. This structure connects the uterus to the vagina.
The main functions of the cervix are related to a woman's fertility:
- It is the orifice through which blood comes out of the uterus during menstruation.
- It allows the entrance of spermatozoa during intercourse.
- It is the baby's exit canal during delivery.
During pregnancy, a woman's body undergoes many changes to adapt to this new situation, including those affecting the cervix.
Provided below is an index with the 7 points we are going to expand on in this article.
- 1.
- 2.
- 3.
- 3.1.
- 3.2.
- 4.
- 4.1.
- 4.2.
- 4.3.
- 5.
- 6.
- 7.
Evaluation of the cervix
During a woman's menstrual cycle, the cervix may undergo minor changes as a result of hormone levels. These changes refer to the following parameters:
- Orifice size
- open cervix or closed cervix depending on the degree of dilatation.
- Consistency
- hard cervix or soft cervix.
- Position
- high cervix (posterior or withdrawn from the vagina) or low cervix (further into the vagina).
For example, during menstruation and ovulation, the cervix is more open to allow blood to flow out and sperm to enter, respectively. On all other days of the menstrual cycle, the cervix will be closed.

Similarly, at the beginning of pregnancy, the cervix may also undergo some changes that will vary from one woman to another. For this reason, the position of the cervix is not a reliable indicator of pregnancy.
Changes of the cervix in early pregnancy
Changes in the cervix during the first weeks of pregnancy should be evaluated by the gynecologist at the consultation.
Most of these changes have to do with the position and texture of the cervix. These are discussed below:
- Cervical softening due to increased estrogen.
- The cervix becomes cyanotic (blue) and increases in volume due to vascularization, swelling and hyperplasia of the cervical glands.
- The cervix rises slightly toward the uterus in the first weeks of pregnancy.
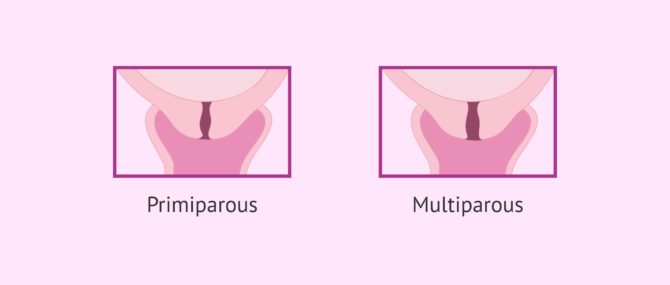
- The internal and external orifices of the cervix are closed in women experiencing their first pregnancy (primigravid) and slightly ajar in those who have already given birth (multiparous).
- The cervical canal becomes fusiform and fills with a thick secretion from the hypertrophied endocervical mucous glands: the mucous plug.
All these changes in the cervix are accentuated as gestation progresses and until the third trimester, at which time the cervix will begin to prepare for delivery.
The mucus plug that forms after conception has a protective function, as it serves to seal the cervical canal and prevent microorganisms and more sperm from entering the uterine cavity during pregnancy.
Position of the cervix during labor
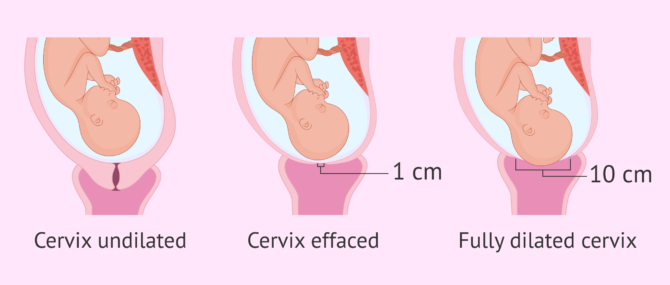
The first stage of labor before delivery is known as dilatation of the cervix dilatation of the cervix.
This stage can last several hours and ranges from the onset of contractions to full dilation of the cervix, which is usually about 10 cm.
Next, we will discuss the changes in the cervix during labor:
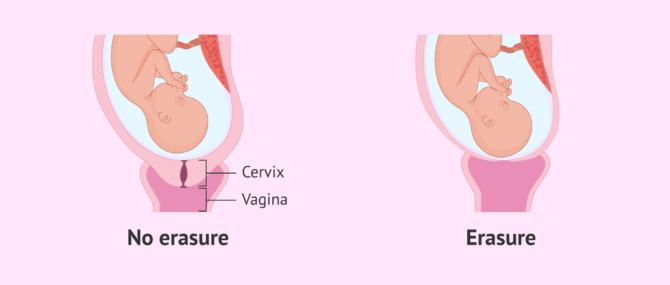
Cervical effacement
The effacement of the cervix corresponds to the early or latent dilatation phase.
This stage means that the cervix is progressively shortening as a result of labor contractions. It is also possible to refer to the effacement of the cervix with the term maturation.
In general, effacement of the cervix does not occur until the day of delivery and has a very variable duration, from 2 to 8 hours.
However, this shortening may begin to occur days earlier due to irregular contractions that are painless and imperceptible to the woman.
In new mothers, the cervix usually takes longer to completely efface, as it is the first time the body is confronted with this process.
In addition to contractions, another symptom of uterine effacement is the expulsion of the mucus plug in the form of a very thick, viscous discharge.
Active dilatation
The cervix is now completely effaced, has the shape of a ring and is now beginning to increase in diameter. The contractions become more frequent and stronger, causing the cervix to open.
The collagen fibers that form it are rearranged, so that their resistance decreases drastically and this facilitates dilatation up to 10 cm. It should be noted that in multiparous women, effacement of the cervix and dilatation of the cervix occur simultaneously. However, in first-time pregnant women, there are two different phases: first the effacement takes place and then the dilatation.
At this time, the cervix also changes position: it moves from being in a posterior position to being centered, so as to facilitate the baby's exit.
Once dilation is complete and the cervix is effaced, the vagina and uterus form a single duct and delivery will take place.
FAQs from users
Can the cervix change its shape or position?
There are biological differences in the cervix between women, which may cause the cervix to have a different shape or position.
Before pregnancy the cervix is normally rigid and closed. During pregnancy it becomes softer and will decrease in length to facilitate dilatation at the time of delivery.
In women who have not given birth it usually has a pointed appearance and in women who have given birth it is more open.
The position may also vary depending on the position of the uterus or if the uterus has fibroids that may displace it.
What does it mean to have a short cervix in pregnancy?
A shortening or dilatation of the cervix during pregnancy carries a risk of premature delivery. This shortening is caused by contractions that can be due to several factors: uterine malformation, urinary tract infection, infection of the cervix, etc.
Normally, the cervix is long and closed during pregnancy. It is about 3 cm long and, if a shortening is detected, the woman must be on bed rest to prevent the cervix from opening. The doctor may also prescribe medication.
What happens if the cervix opens in pregnancy?
The cervix should only shorten and open during labour contractions. If the cervix is found to be open during pregnancy, without having experienced any contractions, the woman may have an incompetent cervix or cervical insufficiency. This is a cervical abnormality that can lead to repeated miscarriages in the second trimester or premature births.
In the case of an incompetent cervix, the doctor may order a cerclage to avoid the risks mentioned above. A cerclage consists of stitches around the cervix to keep it closed.
Suggested for you
There are some alterations and pathologies related to the cervix that prevent women from carrying a pregnancy to term. If you are interested in reading more about this topic, we recommend you to visit the following post: Female infertility due to a cervical factor.
We make a great effort to provide you with the highest quality information.
🙏 Please share this article if you liked it. 💜💜 You help us continue!
References
Ioana-Claudia Lakovschek, Gerda Trutnovsky, Barbara Obermayer-Pietsch, Daniela Gold. Longitudinal Study of Pelvic Floor Characteristics Before, During, and After Pregnancy in Nulliparous Women. J Ultrasound Med. 2022 Jan;41(1):147-155. doi: 10.1002/jum.15689 (View)
Julia Hutchison, Heba Mahdy, Justin Hutchison. Stages of Labor. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan. 2023 Jan 30 (View)
Nicholas M LeFevre, Ellisa Krumm, William Jacob Cobb. Labor Dystocia in Nulliparous Women. Am Fam Physician. 2021 Jan 15;103(2):90-96.
FAQs from users: 'Can the cervix change its shape or position?', 'What does it mean to have a short cervix in pregnancy?' and 'What happens if the cervix opens in pregnancy?'.





